|
|
|
|
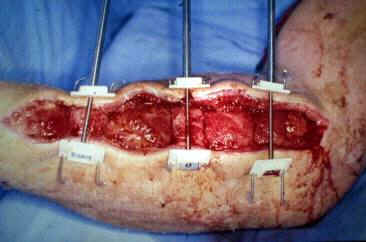
The
use of the original Kirschner wire technique for fasciotomy wound
closure
|
|
|
T.
Molcanyi, *J. Zivcak, M. Kitka, M. Molcanyi, M. Rosak, J.Magdo, **A. Molcanyiova Clinic
of Trauma Surgery, **Department of Clinical Biochemistry, University Hospital of Louis Pasteur, Kosice *Department of instrumental and biomedical engineering, Technical University in Kosice
|
|
| Abstract | |
| Since
1994, the new and original Kirschner-wire technique (KWT) for closure of
fasciotomy wound is used in the Clinic of Trauma Surgery in Košice. The
KWT was used in 29 patients with long bone fractures (4 patients - upper
extremity, 25 patients - lower extremity). In 8 patients, who underwent
a prophylactic fasciotomy after previous arterial injury, the authors
had to combine this technique with the split skin graft (2 patients -
upper extremity, 6 patients - lower extremity). The average age of the
patients was 32,2 years (22 - 55). The average width of the fasciotomy
wound was 5,2cm (4 - 9) on an upper extremity, 10,6cm (5 -16) on a lower
extremity. In the above-mentioned group of 7 patients, the average
intramuscular pressure during the approximation procedure was 35 mmHg
(30-40) and the average CK concentration was 5,6 ukat/l (1,2-8,8). The
average approximation time was 12,2 days (10 - 21). The authors have not
observed neither local inflammation nor systemic signs of myonecrosis
(visceral projection syndrome was not present) in any of the patients.
|
|
| Introduction | |
|
The considerably large number of surgical techniques for closure of the fasciotomy wounds varies one from each other. They can be basically divided into two distinctive groups - different skin-graft techniques and the tension-applying techniques. The closure of the fasciotomy wound should restore both natural compartmental cover and the original compartmental volume. Original prototype – K wires with nylon Modified method – buttons prevent local necrosis |
|
| Subjects and methods | |
|
Since 1994, the new and original Kirschner-wire technique (KWT) for closure of fasciotomy wound is used in our clinic of trauma surgery. First, the K wires are inserted subdermally (transversely to the wound edges) in 2 - 3 cm intervals. They serve as the leading component. The tension for approximating the wound edges is achieved by inserting different plastic pulling clips or binding suture threads onto the K wires. We start the approximation of the wound edges 7-10 days after the fasciotomy, after the edema has begun to resolve. The approximation is carried out in operating room in 2-day intervals. During these sessions we controlled the pressure by palpation the muscles during the operation. In 7 patients we measured the intramuscular pressure (IMP), after every approximation using the Whitesides needle technique. Creatine-kinase (CK) levels in blood were controlled 8-12 hours after every approximation. Second modification – protective infusion tubes Currently in use - plastic clamps on the K wires attached to dynamic system |
|
| Results | |
|
The
KWT was used in 29 patients with long bone fractures
(4 patients - upper extremity, 25 patients - lower extremity). In
8 patients, who underwent a prophylactic fasciotomy after previous
arterial injury, we had to combine this technique with the split skin
graft (2 patients - upper extremity, 6 patients - lower extremity). The
average age of the patients was 32,2 years (22 - 55 years). The average
width of the fasciotomy wound was 5,2cm (4 - 9) on an upper extremity,
10,6cm (5 -16) on a lower extremity. |
|
| Discussion | |
|
Open
fasciotomy (full length skin & fascia incisions) is mandatory in
acute compartment syndrome in order to prevent permanent injury to the
soft tissues. There is no skin loss at the time of the fasciotomy but
difficulty in closure of the wound (due to retraction of the skin edges
away from the underlying exposed tissue). |
|
| Conclusion | |
| Our
original method for fasciotomy wound closure, using transversely
inserted leading K wires combined with different traction-elements,
assures the complete restoring of the original compartmental cover and
volume.
Keywords: fasciotomy wound – Kirschner wire technique - intramuscular pressure
|
|
| References | |
|
1. Almekinders LC. Gradual closure of fasciotomy wounds. Orthopaedic
Rev. 1991;20:82. 2. Asgari MM, Spinelli HM. The vessel loop shoelace technique for
closure of fasciotomy wounds. Ann Plast Surg 2000;44:225-9. 3. Berman SS, Schilling JD, McIntyre KE, Hunter GC, Bernhard M.
Shoelace technique for delayed primary closure of fasciotomies. The Am J
Surg 1994;167:435-6. 4. Callanan I, Macey A. Closure of fasciotomy wounds: A technical
modification. J Hand Surg 1997;22B:264-5. 5. Chiverton N, Redden
JF. A new technique for delayed primary closure of fasciotomy wounds.
Injury, Int Care Injured 2000;31:21-4. 6. Cohn BT, Shall J,
Berkowitz M. Forearm fasciotomy for acute compartment syndrome. A new
technique for delayed primary closure. Orthopedic 1986;10:1234. 7. Harrah J, Gates R, Carl J, Harrah JD. A simpler, less expensive
technique for delayed primary closure of fasciotomies. Am J Surg
2000;180:55-7. 8. McKenney MG, Nir I, Fee T, Martin L, Lentz K. A simple device for
closure of fasciotomy wounds. Am J Surg 1996;172:275-7.
9. Molcanyi T, Kitka
M. Acute compartment syndrome induced by prolonged local pressure with
visceral projection syndrome. Uraz Chir 1999;4:18-22. 10. Molcanyi T, Zivcak J, Molcanyi M, Kitka M, Rosak M, Magdo J,
Molcanyiova A. A Kirschner wire technique for fasciotomy wound closure.
Compartment-syndrome update 2001. International Symposium, March 9th –
11th 2001, Irsee Cloister, Germany: 66-67. 11. Narayanan K, Futrell JW, Bentz M, Hurwitz D. Comparative clinical
study of the Sure-Closure device with conventional wound closure
techniques. Ann Plast Surg 1995;35:485-91. 12. Narayanan K, Latenser BA, Jones LM, Stofman G. Simultaneous
primary closure of four fasciotomy wounds in a single setting using the
SureClosure device. Injury 1996;27:449-51. 13. Velhamos GC, Theodorou D, Demetriades D, Chan L, Berne TV,
Asensio J, Cornwell EE, Belzberg H, Stewart BM. Complications and non
closure rates of fasciotomy for trauma and related risk factors. World J
Surg 1997;21:247-53. 14. Wiger
P, Tkaczuk P, Styf J. Secondary wound closure following fasciotomy for
acute compartment syndrome increases intramuscular pressure. J Orthop
Trauma 1998;12:117/21. 15. Zivcak J,
Molcanyi T. Clinical experience with compartment syndrome monitoring.
MicroCAD 99, Miskolc, Hungary, 1999:54-57. 16. Zivcak J, Molcanyi T. Evaluating the signs of compartment
syndrome in limb fractures, the frontiers of medical biophysics of 21st
century, Bratislava, Slovakia, 1999:56-59.
17. Zivcak J,
Molcanyi T, Slosarcik S. Sensing
system for compartment syndrome measurement. Acta Mechanica Slovaca
2000;2:101-106. |
|